Fill Out a Valid Medication Administration Record Sheet Form
Fill Out a Valid Medication Administration Record Sheet Form
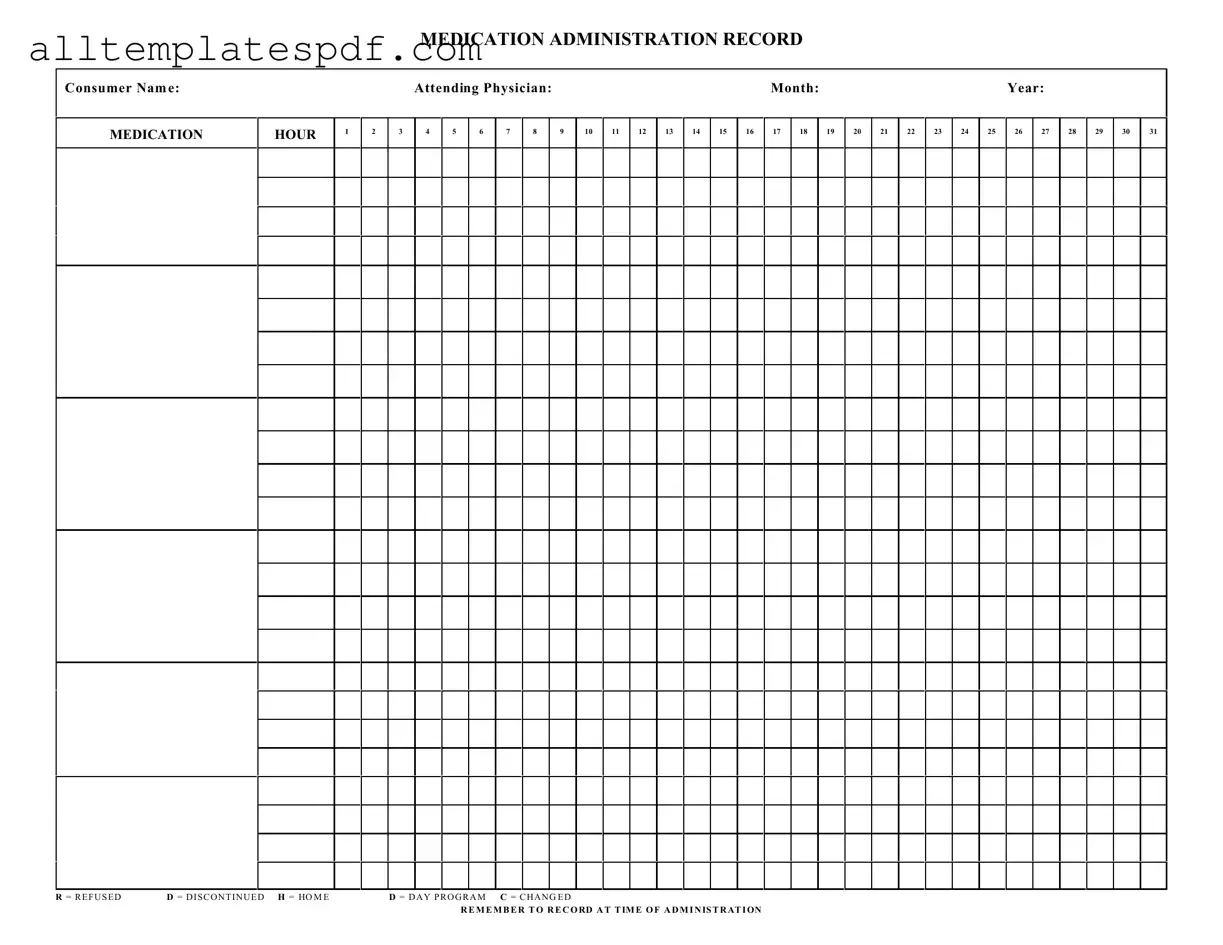
Filling out the Medication Administration Record Sheet is crucial for ensuring proper medication management. However, mistakes can easily occur. One common error is failing to include the consumer's name at the top of the form. Without this essential information, it becomes difficult to track which medications are administered to which individual, leading to potential mix-ups.
Another frequent mistake is neglecting to note the attending physician's name. This detail is important for accountability and communication. If a question arises about a medication, knowing who prescribed it can facilitate quick resolutions and ensure that the right person is contacted.
Many individuals also overlook the importance of accurately recording the date and month on the form. Inaccurate dates can lead to confusion about when medications were administered. This oversight can have serious implications for ongoing treatment plans and medication schedules.
Additionally, some people forget to check off the appropriate boxes for the medication status, such as "refused," "discontinued," or "changed." Each of these indicators provides vital information about the consumer's treatment and adherence to their medication regimen. Missing this step can result in gaps in care.
Lastly, not recording the time of administration is a significant mistake. The instruction to "remember to record at time of administration" is crucial. Accurate timing helps in monitoring the effectiveness of medications and can assist healthcare providers in making necessary adjustments to treatment plans.
Free Job Application Template - It may include a personal statement or cover letter section.
For individuals seeking to navigate the complexities of real estate transactions, our comprehensive guide to the Real Estate Purchase Agreement form is invaluable. This document is essential for safeguarding the interests of both buyers and sellers, ensuring all terms of the sale are clearly defined and legally binding. For more information, visit our helpful resource on Real Estate Purchase Agreement considerations.
Workplace Accident Report - A written account aiding in the prevention of future workplace accidents.
Understanding the Medication Administration Record Sheet (MARS) is crucial for ensuring accurate medication management. However, several misconceptions can lead to confusion. Here are six common misunderstandings:
By addressing these misconceptions, individuals can better utilize the Medication Administration Record Sheet, ultimately enhancing patient care and safety.
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record Sheet is used to document the administration of medications to consumers. |
| Consumer Identification | The form requires the consumer's name to ensure accurate tracking of medication administration. |
| Physician Details | Attending physician information must be included to provide accountability and oversight. |
| Monthly Tracking | The form is structured to track medication administration on a monthly basis, allowing for organized record-keeping. |
| Hourly Administration | It provides designated hours for medication administration, ensuring timely and consistent dosing. |
| Refusal and Discontinuation Codes | Specific codes (R, D, H, C) are used to indicate if a medication was refused, discontinued, administered at home, or changed. |
| Documentation Requirement | It is essential to record the administration of medication at the time it is given to maintain accurate records. |
| State Compliance | In many states, such as California, the use of a Medication Administration Record is governed by the Health and Safety Code. |
| Legal Importance | Proper completion of this form can be critical for legal compliance and protection in case of disputes regarding medication administration. |
Completing the Medication Administration Record Sheet is essential for accurate medication tracking. Follow these steps to ensure all necessary information is recorded correctly.